














 TechMagic Academy
TechMagic AcademyPHI Rules You Must Follow: Legal Requirements, Security Tips, and Common Mistakes to Avoid
Last updated:20 January 2026



In the U.S., the HHS Office for Civil Rights documented 725 large healthcare data breaches in a single year, each affecting 500+ people, the HIPAA Journal reported.
That’s a big number, but what’s more important is what it reflects: even well-intentioned teams can lose control of PHI when workflows speed outruns safeguards.
If you work in healthcare, you’ve likely felt how easy it is for PHI to become a risk. Care teams need to move quickly. Information gets shared across departments, devices, and vendors. Meanwhile, your organization is expected to stay compliant, respond to patient requests, and keep every workflow secure.
That’s why this topic matters. PHI rules shape how you document care, communicate with patients, use modern tools, and stay trusted. And when PHI handling goes wrong, companies face patient harm, reputation damage, regulatory scrutiny, and stressful internal investigations.
In this article, we’ll make PHI rules practical. We’ll clarify what counts as PHI, what the law actually requires, how to secure PHI across workflows, and where organizations make mistakes. You’ll also get a clear PHI rules guide you can use to sanity-check your current practices and reduce risk.
Let’s start!
Key Takeaways
- PHI ≠ just “medical records.” If health information can identify a person, even an appointment note, billing detail, or lab result tied to a name or ID, it’s PHI and must be handled under the right rules.
- Visibility gaps lead to most compliance failures. If you don’t know where PHI lives and how it moves, you’ll miss the biggest risks, especially “shadow PHI” in email, shared drives, screenshots, exports, and personal devices.
- HIPAA sets the baseline, but it’s not the whole picture. Depending on the situation, you may also need to follow stricter state laws, 42 CFR Part 2 for SUD records, FTC breach rules for consumer health apps, and GDPR for EU health data.
- PHI sharing errors often stem from misunderstanding. Many incidents come from misunderstanding what’s allowed outside treatment, payment, and operations, or failing to get proper patient authorization when it’s required.
- Minimum necessary + role-based access reduces risk fast. Narrow access to job needs, review permissions regularly, and avoid broad “everyone can see everything” setups. It protects patients and makes investigations easier.
- Security has to cover the everyday channels. Email, messaging, fax, remote access, and mobile devices are common weak points. If secure options aren’t easy to use, staff will default to whatever is fastest.
- Vendors can create hidden compliance gaps. BAAs are required in many cases, but they’re only the starting point. Due diligence and least-privilege integrations matter just as much.
- Breach readiness is part of compliance. You need monitoring, clear incident response steps, and documentation discipline. When something goes wrong, speed and clarity matter.
What Is PHI and Why Is It Important?
PHI (protected health information) is any health-related information that can identify a person, and it’s protected because it can expose someone’s private life, care decisions, and financial details if mishandled.
Under HIPAA (Health Insurance Portability and Accountability Act), information becomes PHI when it’s individually identifiable and held or shared by a covered entity, like a health care provider or health plan, or their business associate.
PHI isn’t limited to clinical notes or diagnoses. It also includes billing records, lab results, appointment details, insurance information, and even “I saw this patient today” if the person can be identified. The key is the combination: health information + an identifier.
What counts as an identifier?
HIPAA treats many everyday data points as identifying when they can be linked to a patient: things like a name, address, date of birth, phone number, electronic mail address, Social Security number, medical record number, full-face photos, or even web universal resource locators tied to a person or session. Once any of that is attached to health information, it’s generally PHI.
What doesn’t count as PHI?
Two common cases:
- De-identified health information (when identifiers are removed according to HIPAA methods) is not PHI.
- Employment records held by an employer (even if they mention health info) usually aren’t treated as PHI under HIPAA because they’re not part of a covered entity’s healthcare records.
Why PHI is treated differently from other sensitive data
PHI is sensitive for a few reasons:
- It’s personal in a way few other data types are. A credit card can be replaced. A diagnosis, physical or mental health history, fertility treatment, or substance use record can follow someone for life.
- It moves fast. PHI travels across EHRs, labs, imaging systems, claims platforms, portals, secure messaging tools, and vendor integrations.
- It creates real harm when exposed. Beyond regulatory penalties, a PHI breach can lead to discrimination, stigma, loss of employment opportunities, and patients delaying care because they don’t trust the system.
From a cybersecurity perspective, PHI is also a high-value target. Healthcare data is rich, hard to change, and often connected to payment systems, which is one reason healthcare remains such a frequent focus for attackers.
Next, let’s talk about what the law requires, because once you understand the legal baseline, it becomes much easier to prioritize controls and avoid the most common compliance mistakes.

What Are the Legal Requirements for Handling PHI?
The legal requirements for handling PHI come down to three core duties: (1) only use or share PHI in permitted ways, (2) protect it with reasonable safeguards, and (3) notify people and regulators when unsecured PHI is breached.
In the U.S., HIPAA is the baseline, but several other laws and regulators can add stricter rules depending on the data type, the patient population, and whether you’re dealing with consumer health data outside HIPAA.
Now let’s explore the most relevant frameworks and what they mean for day-to-day practice.
HIPAA (privacy, security, and breach notification rules)
HIPAA is the foundation for PHI rules in the U.S., and it defines what PHI is, how it can be used or disclosed, what rights patients have, and what safeguards organizations must implement for ePHI.
Practically, HIPAA breaks down into three HIPAA PHI rules:
- HIPAA Privacy Rule. Sets boundaries for when PHI can be used or disclosed (including the “minimum necessary” expectation) and establishes patient rights such as access to records and an accounting of certain disclosures.
- HIPAA Security Rule. Applies to electronic protected health information (ePHI) and requires administrative, physical, and technical safeguards, including access controls and risk analysis.
- HIPAA Breach Notification Rule. Requires HIPAA covered entities and business associates to provide notifications after a breach of unsecured PHI, following specific timing and reporting rules.
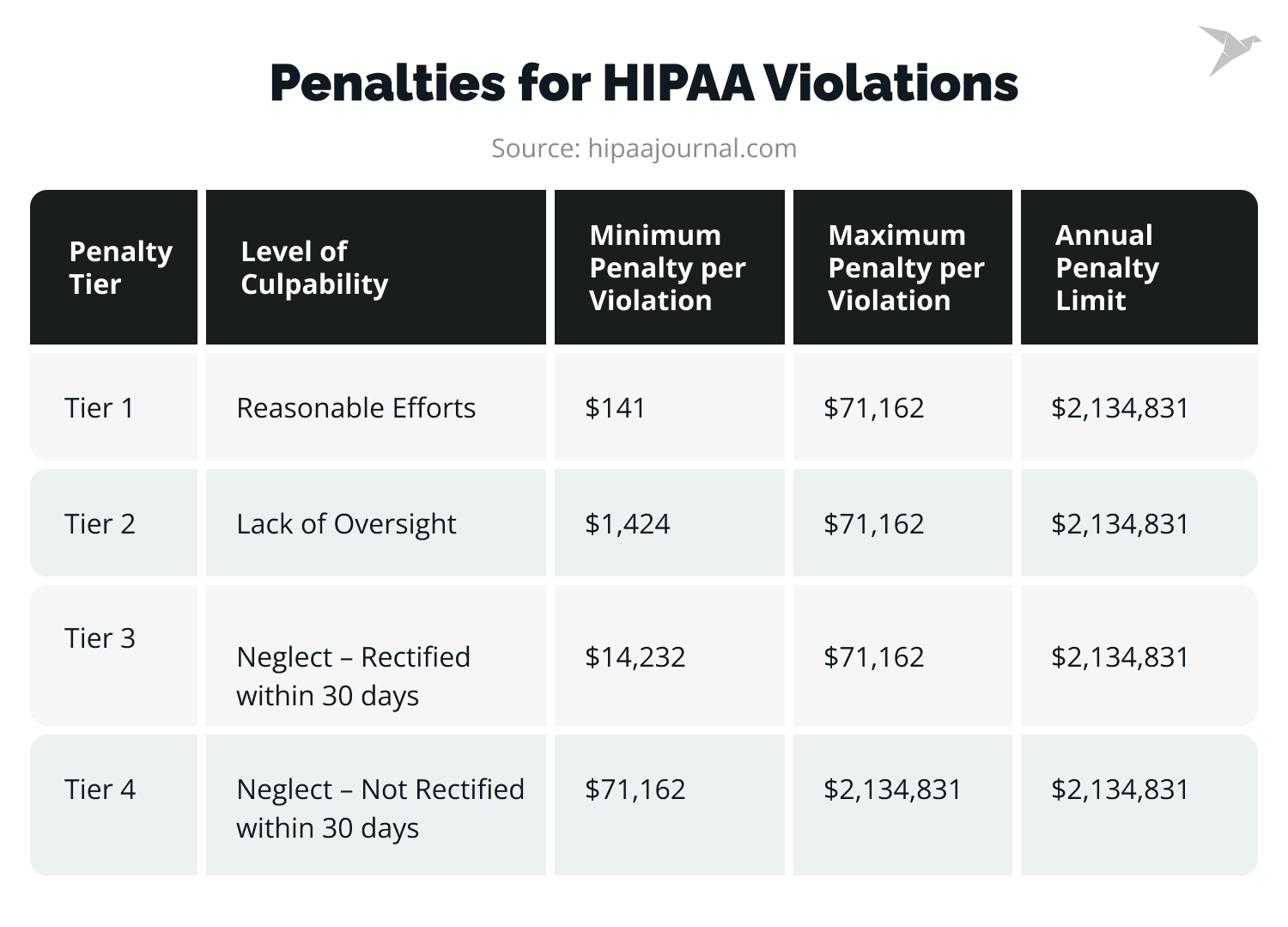
💡 The Health and Human Services Office for Civil Rights ramped up enforcement in 2024: 22 HIPAA enforcement actions (the second-highest ever) were completed, totaling $9.9 million in fines and penalties.
HIPAA doesn’t just care about whether PHI was exposed; it cares about whether you had reasonable safeguards in place and whether you followed the required response steps once you detected a potential breach.
HITECH Act
HITECH strengthened HIPAA by making enforcement sharper, increasing potential penalties, and extending direct compliance expectations to business associates and vendors.
Three practical impacts matter most:
- Bigger penalties and stronger enforcement. HITECH increased enforcement leverage and penalty exposure for noncompliance.
- Mandatory breach reporting mechanisms. It reinforced breach notification obligations and made reporting a central compliance requirement, not an optional best effort.
- Business associate accountability. Vendors handling PHI can be directly accountable for HIPAA compliance failures, which changes how you manage contracts, onboarding, and security reviews.
If you rely on cloud providers, billing services, analytics platforms, telehealth vendors, or outsourced IT, HITECH is a big reason you can’t treat vendor risk as a side issue.
42 CFR Part 2 (stricter rules for substance use disorder records)
42 CFR Part 2 sets stricter confidentiality rules for substance use disorder (SUD) treatment records than HIPAA, including tighter consent requirements and limits on redisclosure. It exists because SUD records carry a high risk of stigma and discrimination, and the law aims to reduce that harm.
For integrated care teams, Part 2 is where “PHI rules” get more complex. Even if you have strong HIPAA processes, SUD records may require more explicit consent controls and careful handling in shared EHR environments.
State Privacy and Health Data Laws (when state rules override HIPAA baselines)
HIPAA is the federal minimum standard, but state privacy and health data laws can be stricter, and when they are, you must follow the more protective rule.
This often shows up in rules around:
- Mental/behavioral health records
- HIV/STI status
- Genetic information
- Minors’ records and consent
For compliance officers and administrators, this is one of the hardest areas because it’s not always obvious when a state rule “wins.” It’s also where policy templates can mislead you: what’s compliant in one state may be insufficient in another.
FTC Health Breach Notification Rule (health apps and consumer health data outside HIPAA)
The FTC Health Breach Notification Rule applies to many health apps and personal health record (PHR) vendors that aren’t covered by HIPAA, and it still requires breach notification when unsecured individually identifiable health information is exposed.
Simply put, if your organization works with consumer-facing health tools outside the HIPAA ecosystem, you can still have legal notification obligations.
Key points:
- It covers vendors of personal health information records and related entities, and it also affects their service providers.
- Notifications may need to go to individuals, the FTC, and sometimes the media, depending on scale.
- Enforcement attention is growing, and the rule was modernized in 2024, which is why it’s showing up more often in health tech compliance conversations.
This matters for hybrid orgs. For example, providers partnering with wellness apps, remote monitoring tools, or patient engagement platforms that don’t neatly fit HIPAA definitions.
Medicare/Medicaid and CMS Compliance Requirements (operational rules that shape PHI practices)
CMS participation and reimbursement rules don’t always sound like “PHI law,” but they strongly influence PHI handling through documentation requirements, patient access expectations, and operational compliance standards.
For administrators, the practical risk lies in noncompliance, which can mean audits, corrective action plans, or consequences tied to program participation.
Even when HIPAA is your core privacy framework, CMS expectations often shape the real workflows: how records must be maintained, how access is provided, and how integrity is protected.
FDA and Clinical Research Rules (when PHI is used in trials or medical device/software workflows)
When PHI is used in clinical research or medical device/software validation, additional privacy and consent expectations may apply beyond standard care workflows. In research settings, PHI handling may be governed by informed consent requirements and oversight mechanisms such as IRBs, depending on the study and context.
This is most relevant if your organization runs registries, studies, or develops regulated software/device workflows. If you’re purely focused on clinical care operations, we can keep this as a lighter note, but it’s important for many healthcare orgs with research arms.
HHS OCR Guidance and Enforcement (how legal requirements are applied in the real world)
HHS OCR guidance and enforcement actions are where “legal requirements” become real expectations, especially for modern workflows like cloud systems, remote work, telehealth, and messaging.
OCR enforcement tends to focus on patterns such as:
- Weak risk analysis practices
- Gaps in access control and auditability
- Delayed breach response
- Insufficient safeguards around common tools (email, mobile devices, third-party platforms)
In other words, regulators often judge whether you applied reasonable safeguards, not whether you had a policy document on paper.
GDPR and Special-Category Health Data (if you handle EU patient information)
If you handle EU patient information, GDPR treats health data as “special category” personal data, which triggers stricter processing rules and security expectations. That can affect everything from lawful basis and transparency requirements to data minimization and cross-border transfer controls.
Even U.S.-based healthcare providers and vendors can run into GDPR obligations when EU residents’ data is involved, especially in telehealth and cross-border care arrangements.
National Health Data Laws Outside the U.S.
Outside the U.S., PHI-equivalent data is typically regulated under national health privacy and data protection laws, and the details vary by country. If your organization operates internationally or serves patients across borders, you’ll usually need a layered compliance approach: local health data rules + general privacy law + security controls that meet the strictest applicable standard.
Now that the legal baseline is clear, the next step is exploring the required security measures and operational controls.
How Should You Secure PHI in Your Organization?
You secure PHI by combining administrative, technical, and physical safeguards and making sure they work in real clinical workflows. The most effective programs reduce unnecessary access, encrypt data everywhere it travels, guide staff toward safe communication habits, and build the ability to detect and respond quickly when something goes wrong. Now let’s explore what that looks like in practice.
PHI risk assessment to know where PHI lives
A PHI risk assessment must be the first step, because you can’t secure PHI you haven’t mapped. It should capture where PHI is created, stored, accessed, and shared, and where it leaks into “unofficial” spaces.
In most organizations, PHI touches the electronic health records, imaging, labs, billing, patient portals, and analytics tools. But the bigger risk often is in those systems: email attachments, shared drives, screenshots added to tickets, chat threads, printed documents, and personal devices used during busy shifts. A solid assessment shows PHI movement across workflows, endpoints, and vendors, so you can close gaps without breaking care delivery.
Administrative safeguards
Administrative safeguards include policies, roles, and training that reduce the most common PHI risk: human error. Start with policies and procedures that match how your teams actually work, especially around communication and access. Assign clear privacy and security responsibility to people who can make decisions and resolve recurring issues.
Then, make training practical: short refreshers, role-based examples, and clear guidance on everyday scenarios like sending records, using messaging, handling patient requests, or dealing with a lost device. Compliance also expects accountability, so violations need a defined response. Not because teams want to punish mistakes, but because consistent enforcement reduces repeat risk.
Technical safeguards
Technical safeguards protect ePHI by controlling access, confirming identity, and keeping a reliable record of activity. They’re also how you detect problems early and prove compliance later.
At minimum, you want unique user IDs, strong authentication (including MFA where feasible), role-based access, and automatic session timeouts, especially in shared workstation settings. Audit logs matter just as much as prevention.
If you can’t reliably answer “who accessed what, when, and why,” you’ll struggle during investigations, audits, and breach assessments. Monitoring doesn’t need to be complex to be useful. Even basic alerting on unusual access patterns can prevent small issues from becoming reportable events.
Encryption for PHI at rest and in transit
Encryption is one of the most effective safeguards because it lowers breach impact when devices are lost, stolen, or intercepted. In addition to production databases, it should cover data at rest, data in transit, and backups.
For most organizations, the weak spots are endpoints and portable storage. Laptops, phones, and removable media still show up in breach reports because loss and theft are predictable events.
Encrypt devices by default, enforce it through management tools, and make sure backups are encrypted and access-controlled as tightly as the health care systems they protect. Transmission matters too: PHI should move through secure channels (TLS for system-to-system traffic, and approved secure solutions for communication).
Secure PHI sharing
Ensuring security while PHI sharing can be hard because speed and habit tend to override policy. The fix is giving people secure options that are actually usable.
For email, that usually means encryption or secure portals, plus controls around forwarding and attachments. For texting and messaging, approved platforms should support auditability and access control, otherwise you lose visibility and may create retention problems.
Faxing still needs safeguards too: verification steps, misdial prevention, cover sheets, and secure placement of machines so pages aren’t sitting in public view. Patient communication is also complex. If a patient requests an insecure method, you often can honor it, but you need a documented request and a clear process so staff aren’t making that call on the fly.
💡 There is also a public wariness about new technologies like AI. 37% of Americans believe that greater use of AI in healthcare will worsen the security of patients’ records, while only 22% think AI would improve health data security, Pew Research Center reported.
Device and endpoint security
Device and endpoint security management processes cover workstations, laptops, smartphones, and tablets. Endpoints are where PHI meets the real world and where attackers and accidents usually start. The goal is consistent controls across every device that can access or store PHI.
Encryption, automatic screen lock, and patching are table stakes. Mobile devices should be managed through MDM, with remote wipe capability and app controls that prevent PHI from being stored in the wrong place. Vulnerability management should be routine, because unpatched endpoints are still one of the easiest ways for attackers to get a foothold. If BYOD exists, define strict boundaries. Without them, PHI spreads across personal apps and unmanaged storage faster than any policy can catch up.
Physical safeguards
PHI security is also physical, because privacy failures often happen in hallways, nursing stations, printers, and shared spaces. Many “small” incidents start here: a chart left on a desk, a screen visible to visitors, or pages left at a shared printer.
Strong physical safeguards include controlled physical access to areas where records are stored, workstation placement that minimizes casual viewing, secure printing practices, locked storage for paper records, and proper disposal through shredding or secure destruction. These controls aren’t glamorous, but they prevent the most avoidable disclosures.
Minimum necessary access and role-based permissions
Minimum necessary access reduces PHI exposure by design, and it’s one of the fastest ways to cut risk without adding friction. The idea is that access should match job duties, not convenience.
This works best when roles are clearly defined, permissions are tiered (view vs. edit vs. export), and access reviews happen regularly, especially after job changes or when staff leave. Broad access to the entire EHR may feel efficient, but it increases the blast radius of both insider misuse and compromised accounts.
The more you can narrow access while keeping care efficient, the more resilient your program becomes.
Vendor and cloud security
Vendor security is critical because PHI often flows through third parties, and your organization still carries responsibility for that exposure. A BAA is necessary where required, but it’s not enough on its own.
💡 In 2024, business associates were responsible for only 16% of reported breaches but a staggering 66% of all compromised healthcare records, according to Bluesight 2025 Breach Barometer.
You also need due diligence: understand what PHI the vendor touches, what security controls they have, and what evidence they can provide (SOC 2, ISO 27001 where relevant, penetration testing summaries, incident history).
Cloud adds a shared responsibility layer. You need clarity on who handles identity controls, encryption, logging, backups, and incident response. Integration design matters too. Many avoidable exposures happen when tools are granted broad access because “it was easier” during implementation.
Incident response and breach readiness
PHI security includes being ready for incidents, because strong controls reduce risk, but they don’t eliminate it. What matters is how quickly you detect, contain, assess, and document what happened.
A breach-ready organization has a clear incident response plan, a reporting workflow that staff can use without fear, and a defined process for breach risk assessment. Legal and compliance should be involved early, so the team can meet notification requirements without chaos. The biggest operational pain point is usually delay: waiting too long to escalate, investigate, or document decisions. Clear workflows prevent that.
Ongoing monitoring, auditing, and continuous improvement
PHI security is ongoing work. Workflows evolve, staff changes, and new vendors appear, and each change introduces new exposure.
Sustainable programs review audit logs, monitor for unusual access, run periodic assessments, and test staff readiness with phishing simulations and targeted refreshers. Vulnerability scanning and patch cycles should be predictable and owned. Over time, the goal is fewer exceptions, fewer unknowns, and fewer “surprises” when an audit or incident happens.
Data retention and secure disposal
PHI should be kept only as long as required, and disposed of so that it can’t be recovered. Over-retention increases breach exposure and expands what you must review during audits, incidents, or legal requests.
Set a retention schedule that aligns with federal and state rules, payer requirements, and internal needs. Apply it across primary systems and the places PHI quietly accumulates: exports, shared drives, emails, archived reports, backups, and test environments.
Disposal needs to be verifiable. Paper requires secure destruction. Electronic PHI requires secure deletion or media sanitization (not just “delete”). Old devices and drives should be wiped or destroyed with documentation, since retired hardware is a frequent source of accidental disclosure.
Secure remote work and telehealth
Remote work and telehealth are manageable, but they raise PHI risk unless devices, access, and privacy are tightly controlled. Most issues come from everyday gaps: shared spaces, unsecured networks, and unmanaged endpoints.
Use approved devices, enforce MFA, and secure remote access (VPN or equivalent). Prevent local PHI storage where possible, require screen locks, and use remote wipe for lost devices. Staff also need clear rules for privacy in shared environments, including what to do when others can see or hear PHI.
💡 In a 2024 survey of tele-mental health patients conducted by Propeller Insights, 35% reported that their telehealth sessions were not HIPAA-compliant or secure, and an overwhelming 92% expressed concerns about the privacy and security of their sessions.
For telehealth platforms, focus on access control, encryption, auditability, and vendor obligations (including BAAs where required). Pay special attention to recordings, transcripts, chat logs, and file-sharing features as these often become untracked PHI repositories.
Now that we’ve covered how to secure PHI in day-to-day operations, let’s clarify the key PHI rules that govern how it can be used, accessed, shared, and documented.
What Are the Key Rules of PHI?
The key PHI rules are the practical “do’s and don’ts” that tell you when PHI can be used or shared, how to secure it, and what you must document to prove compliance. Most requirements come down to permitted use/disclosure, minimum necessary access, safeguards for ePHI, patient rights, vendor controls, and breach response obligations. Now let’s break those key PHI rules down one by one.
Only use or disclose PHI for permitted purposes
PHI may only be used or disclosed when the law permits it. Most commonly for treatment, payment, and healthcare operations (TPO), or when another specific HIPAA permission applies. Anything outside those boundaries (for example, disclosing protected health information to a third party for reasons unrelated to care or payment) requires a clear legal basis, and in many cases, patient authorization. This rule is the core of most PHI and HIPAA rules because it defines what “allowed” actually means.
Obtain valid patient authorization when required
Some uses and disclosures require explicit, written patient authorization, especially those outside TPO, including many marketing-related disclosures and non-routine sharing. An individual's authorization must be specific (what data, who receives it, why, expiration) and must be retained as part of your compliance evidence. If an organization can’t produce the authorization later, the disclosure often becomes a compliance problem, even if the intention was harmless.
Follow the “minimum necessary” rule
The minimum necessary rule means you should access, use, or disclose only the minimum amount of PHI needed to complete a task, particularly for administrative work like billing, reporting, analytics, and third-party requests. This is one of the top PHI rules because it reduces exposure even when sharing is legally permitted.
Apply role-based access controls (PHI access must match job duties)
PHI access should be based on role and necessity. Role-based access control (RBAC) supports minimum necessary by design, and it’s a common focus area during audits and investigations. When roles are too broad, organizations often find inappropriate access patterns they didn’t intend, and can’t easily justify after the fact.
Secure PHI in any form (electronic, paper, verbal)
PHI rules apply regardless of format. That includes ePHI in systems and devices, paper records and printed materials, and verbal PHI that can be overheard in public or semi-public spaces. Many compliance issues are preventable disclosures through screens, printers, hallway conversations, or documents left in the wrong place. A strong PHI rules guide always treats physical and verbal privacy as a real risk.
Protect ePHI with required safeguards
The HIPAA Security Rule protects ePHI, requiring safeguards across three areas: administrative (policies, training, risk analysis), physical (facility and device controls), and technical (access control, audit logs, transmission security). Safeguards must actually be implemented and maintained, not just documented. If ePHI is accessed remotely, stored in the cloud, or shared across vendors, those safeguards need to extend into those workflows.
Document policies, training, and compliance activities
PHI compliance must be provable. Organizations should maintain written privacy and security policies, training records, risk analyses, corrective actions, and documentation of incident investigations and decisions. If something goes wrong, regulators will often look at what you did before the incident (risk analysis, safeguards, training) and how you responded after it (documentation, remediation, notification logic). Clear documentation also helps you distinguish mistakes from patterns that can rise to HIPAA violations.
Use BAAs before sharing PHI with vendors
If a vendor handles PHI on behalf of a covered entity, a Business Associate Agreement is required before PHI is shared. A business associate is any person or organization performing services that involve PHI. For example, cloud hosting, billing, analytics, transcription, or certain IT support. A BAA defines permissible use, required safeguards, breach reporting responsibilities, and limits on further disclosure. No BAA is a major compliance risk, even if the vendor “seems secure.”
Report and respond to PHI breaches within required timelines
Suspected incidents involving PHI must be evaluated quickly, documented, and escalated through a defined breach assessment process. If a breach is confirmed, notifications must follow legal timelines and scope: to affected individuals, regulators, and sometimes the media, depending on impact size. Delayed detection, unclear internal reporting, and incomplete documentation are common reasons that breach response becomes chaotic.
Provide individuals with their legal rights over PHI
Patients have enforceable rights over their PHI, including the right to access and obtain copies, request amendments (with limits), and receive required privacy notices. In some cases, they can request an accounting of certain disclosures. Healthcare organizations need operational workflows to fulfill these requests within required timelines and in required formats. Failure here is often less about technical security and more about process maturity and staff training.
Next, let’s look at the most common PHI compliance mistakes that show up repeatedly in real audits, incident reviews, and breach investigations, and explain how to prevent them.

What Are the Common Mistakes in PHI Compliance?
Most PHI compliance failures come from predictable operational gaps: limited visibility into PHI, inconsistent sharing practices, weak vendor controls, and delayed detection or response. These issues require clear guardrails, usable processes, and accountability. Now, let’s break down the most common mistakes and the simplest ways to prevent them.
Not knowing where PHI lives or “shadow” PHI
Problem: PHI often spreads beyond the EHR into email threads, shared drives, downloaded exports, screenshots, and personal devices. Once it’s outside controlled systems, access is harder to track, retention becomes messy, and a small incident (lost laptop, wrong share link) can lead to a reportable breach.
Solution: Maintain a living PHI inventory and map PHI flows by workflow (intake, referrals, billing, care coordination). Limit downloads and exports where possible, lock down shared drives, and require approved tools for sharing. If BYOD is allowed, use MDM and clear rules that prevent local PHI storage.
Misunderstanding when PHI can be shared
Problem: Teams may assume “it’s for a good reason” is enough to share PHI. But HIPAA permissions are specific, and disclosures outside treatment, payment, and operations can require patient authorization or other legal justification. This is where PHI disclosure rules are often misunderstood, especially with third parties, family members, employers, or external service providers.
Solution: Train staff on a simple decision model: “Is this TPO? If not, what’s the legal basis?” Provide quick-reference guidance for common scenarios (care coordination, referrals, patient requests, and third-party asks). Build workflows that require authorization documentation when needed.
Sending PHI to the wrong recipient
Problem: Misaddressed email, auto-complete mistakes, wrong fax numbers, and sending to the wrong chat thread are everyday errors, and they’re one of the most common breach triggers because the disclosure is immediate and hard to reverse.
Solution: Use secure messaging tools with directory controls and auditability. Configure email safeguards (warnings for external addresses, encryption rules, restricted forwarding). For fax, require verification steps and use pre-programmed numbers for frequent recipients. Create an “oops protocol”, so staff report mistakes immediately, before the situation escalates.
Using non-compliant vendors or tools
Problem: A tool may look “secure,” but if it handles PHI and you don’t have the right agreements and controls, it becomes a compliance risk. Missing BAAs, unclear subcontractors, or vendors without basic security evidence can put your organization in a weak position during incidents and audits.
Solution: Treat vendor onboarding as a PHI gate. Confirm whether the vendor is a business associate, sign BAAs before sharing PHI, and perform due diligence (security documentation, audit reports where applicable, incident history, access controls, encryption, logging). Restrict vendor access to only what they truly need.
Missing breaches because nobody monitors access or alerts
Problem: Organizations can’t respond to what they don’t detect. Without monitoring, compromised accounts, inappropriate access (“snooping”), and misconfigured systems can go unnoticed until a patient complaint, media report, or external investigation forces action.
Solution: Enable audit logs and review them routinely, especially for high-risk systems like EHRs, imaging, and portals. Set alerts for unusual patterns (mass export, after-hours access, access to VIP records, repeated failed logins). Make investigation procedures clear so teams don’t hesitate or improvise.
Assuming de-identified data is automatically safe
Problem: Teams sometimes treat “de-identified” as a magic label. In reality, data can be re-identified, especially when combined with other datasets or when small populations, rare conditions, or detailed dates and locations remain. Incorrect de-identification can create legal and reputational risk.
Solution: Use formal de-identification approaches aligned with HIPAA regulations (and document your method). Limit detail to what’s truly needed, assess re-identification risk when sharing externally, and apply governance controls to analytics datasets the same way you would to PHI.
Mishandling sensitive records with stricter rules (SUD, mental health, HIV/STI, minors)
Problem: Some data categories carry stricter consent and disclosure rules than general HIPAA. Substance use disorder records under 42 CFR Part 2 are a common example, and many states add extra protections for mental health, HIV/STI status, genetic data, and minors’ records. A disclosure that’s “fine under HIPAA” can still be noncompliant under stricter rules.
Solution: Identify sensitive categories early and build segmentation where possible (role-based access, consent workflows, redisclosure controls). Train staff on what counts as “special category” data in your state and when escalation is required. If your EHR supports it, use flags or labeling to prevent accidental sharing.
Weak incident response and late notification
Problem: Even strong safeguards won’t prevent every incident. The failure happens when the organization delays escalation, lacks a clear breach assessment process, or can’t document decisions. Late detection and messy response often increase harm and regulatory exposure more than the original incident.
Solution: Maintain a tested incident response plan with defined roles, escalation paths, and breach assessment steps. Make reporting easy and non-punitive so staff speak up quickly. Involve privacy, security, and legal early, and prepare notification workflows in advance (templates, contact lists, and timelines) so you’re not building the process during a crisis.
Want a Clear, Secure PHI Compliance Plan You Can Actually Run?
PHI rules are clear on paper. Making them work across real systems, real staff habits, and real vendor ecosystems is the hard part. If you’re dealing with messy PHI flows, inconsistent access controls, or pressure to move faster than your safeguards, it helps to have a team that understands both healthcare workflows and security engineering.
TechMagic builds secure healthcare software and supports organizations with HIPAA-compliant healthcare software development services. Security isn’t a separate step for us. Our developers work alongside security specialists, so encryption, access control, auditability, and vendor boundaries are designed into the product and the integrations from the start. That means fewer workarounds, fewer gray zones, and fewer unpleasant surprises during audits or incident reviews.
Need reassurance before moving forward? Our HIPAA consulting services can help you validate your PHI compliance approach and define a clear, prioritized plan.
Let’s discuss how we can help you!
Wrapping Up and Where PHI Compliance Is Heading Next
To wrap this up, PHI compliance comes down to a clear set of priorities: understand where PHI lives and how it moves, share it only when allowed, limit access to what’s necessary, secure PHI in every form, and keep the documentation and auditability to prove it. When these pieces are in place, issues are easier to prevent, detect, and resolve.
In the next few years, PHI protection will be shaped by three clear trends. First, more PHI will move outside traditional clinical systems into cloud platforms, patient apps, remote monitoring tools, and vendor integrations. Second, remote work and telehealth will keep raising the bar for identity, device security, and privacy in non-clinical environments. Third, enforcement will continue to focus on practical safeguards like access control, monitoring, and timely breach response. The smartest move now is to treat PHI security as part of daily operations and revisit controls regularly as workflows and vendors change.
FAQ

Protected health information (PHI) is any health-related information that can identify a person. It includes clinical details (diagnoses, test results), administrative data (appointments, billing), and anything else tied to an identifier like a name, date of birth, medical record number, or contact details.
You’re compliant when you can show that PHI is used and disclosed only as allowed, protected with required safeguards, and supported by documentation and monitoring. In practice, that means you have a current risk assessment, role-based access controls, secure communication methods, BAAs with vendors, staff training records, audit logs, and a tested incident response process.
PII is any information that identifies a person, while PHI is sensitive health information that identifies a person and is protected under healthcare privacy rules. A name or email is PII; that same name tied to a diagnosis, appointment, lab result, or health insurance coverage claim becomes PHI in a HIPAA-covered context. PHI is usually treated as more sensitive because it reveals health status and care history.
Act fast: contain the issue, preserve evidence, assess what data was exposed, and start a documented breach risk assessment. Notify your privacy/security leads immediately, involve legal/compliance early, and follow breach notification rules based on the scope and whether the PHI was unsecured. Even suspected breaches should be investigated and documented. Delays are a common reason breaches escalate.

