














 TechMagic Academy
TechMagic AcademyHow To Achieve Interoperability in Healthcare: A Practical Guide for 2026
Last updated:4 February 2026


Only 8% of physicians report “ideal interoperability” for test results from outside health systems, according to the Jama Network. And even for encounter documents, it tops out at 19%.
Interoperability is one of those words that may sound simple until you’re the one owning it. You’ve got clinicians who need clean data in the workflow, executives who want measurable ROI, and compliance experts watching every data movement. Meanwhile, the reality is messy: multiple EHRs, labs, imaging, pharmacy, claims, patient apps, and partner networks, all speaking slightly different languages.
In 2026, interoperability is measured by what it enables.
- Can a clinician trust what shows up in the chart?
- Can a patient pull their records without a support ticket?
- Can you add a partner system without another six-month interface project?
- And can you do all of that while staying secure, auditable, and compliant?
This guide of achievement interoperability in healthcare lays out what interoperability means now, who needs it most, the problems it solves, which standards matter in 2026, how to design an architecture that scales, and the implementation traps that quietly derail projects.
Key Takeaways
- Interoperability is judged at the point of care. If data from labs, imaging, medications, and history doesn’t appear in a usable form, clinicians are left with gaps.
- Usable data is the goal. Interoperability means data can be applied in workflows without manual cleanup.
- Different stakeholders want different outcomes. Providers want continuity, payers want automation, vendors want repeatable integrations, IDNs want consistency, and compliance teams want control.
- Most value is in daily operations. Interoperability cuts duplicate tests, reduces re-entry, speeds referrals, and aligns clinical and billing data.
- Standards matter, but only if implemented well. HL7 v2 still runs core flows; FHIR and SMART power APIs and apps; profiles and IHE reduce ambiguity; terminology gives data meaning.
- Architecture determines whether you scale. Integration layers, API gateways, events, and contracts reduce breakage and contain change.
- Identity, terminology, and security come first. MPI, normalization, least-privilege access, consent, and audit trails can’t be bolted on later.
- Most failures are predictable. Data quality, vendor limits, workflow edge cases, unclear ownership, and weak metrics derail efforts to achieve interoperability in healthcare.
What Is Healthcare Interoperability in 2026?
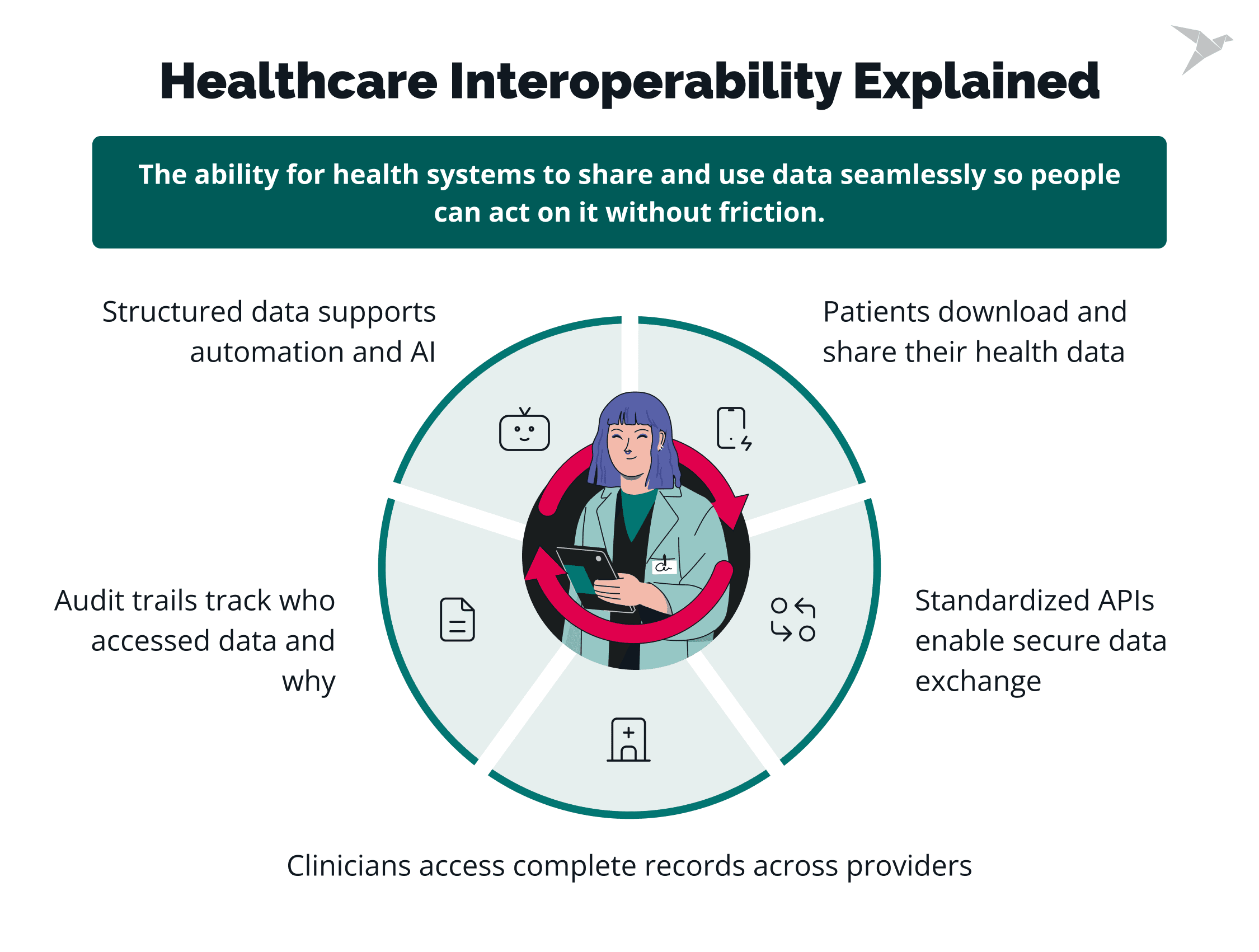
Healthcare interoperability in 2026 is the ability to exchange and use health data reliably, securely, and meaningfully across systems and care settings so that clinicians, patients, and partners can act on that data with minimal effort.
In practice, interoperability means:
- A clinician opening a patient chart and seeing the latest labs from outside facilities.
- Automated eligibility checks and prior auth without manual uploads.
- Patient portals that actually let patients download and share their records.
Regulatory pressure has intensified attention
Recent mandates in the U.S., Europe, and other regions now require not just data availability but API-based access with defined semantics and audit trails. That shifts the bar:
- Healthcare organizations must deliver consistent, standardized data to patients and partners.
- Blocking access without a legitimate reason is increasingly penalized.
- Documentation and evidence of compliance are expected at audit time.
Those pressures have accelerated real adoption of standards like FHIR, SMART on FHIR, and national profiles.
Patient expectations must be met
Patients now expect data access the same way they expect banking or travel booking apps to work:
- Immediate access to records
- Portable data for new providers
- Control over data sharing
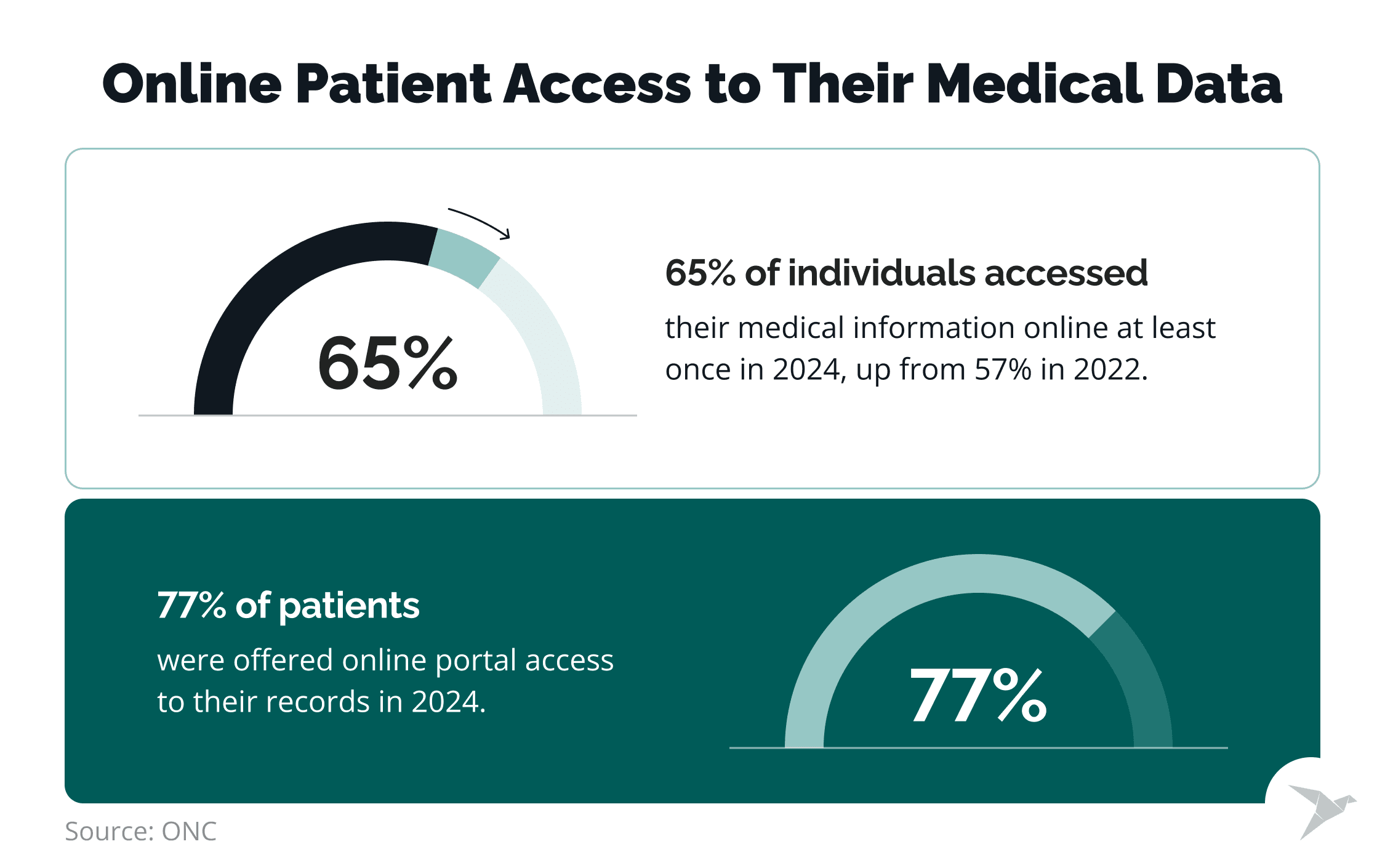
💡 Recent data by ONC confirms this: 65% of individuals accessed their medical information online at least once in 2024 (up from 57% in 2022), and 77% of patients were offered online portal access to their records in 2024. Clearly, digital access to health data is becoming the norm.
AI-driven care has changed what “good enough” looks like
Artificial intelligence and advanced analytics in healthcare depend on consistent, normalized, and high-quality clinical data. Achieving this requires semantic interoperability, which ensures that different systems share a standardized, meaningful understanding of data. AI can help interpret complex data formats and improve medical record retrieval, but gaps, duplicates, or ambiguous codes break models and erode trust. Interoperability in 2026 means:
- Structured data flows
- Terminology normalization so that systems “speak the same language”
- Metadata, context, and provenance that support automation
Next, let’s explore who actually needs interoperability and why it matters to them.

Who Actually Needs Interoperability – and Why?
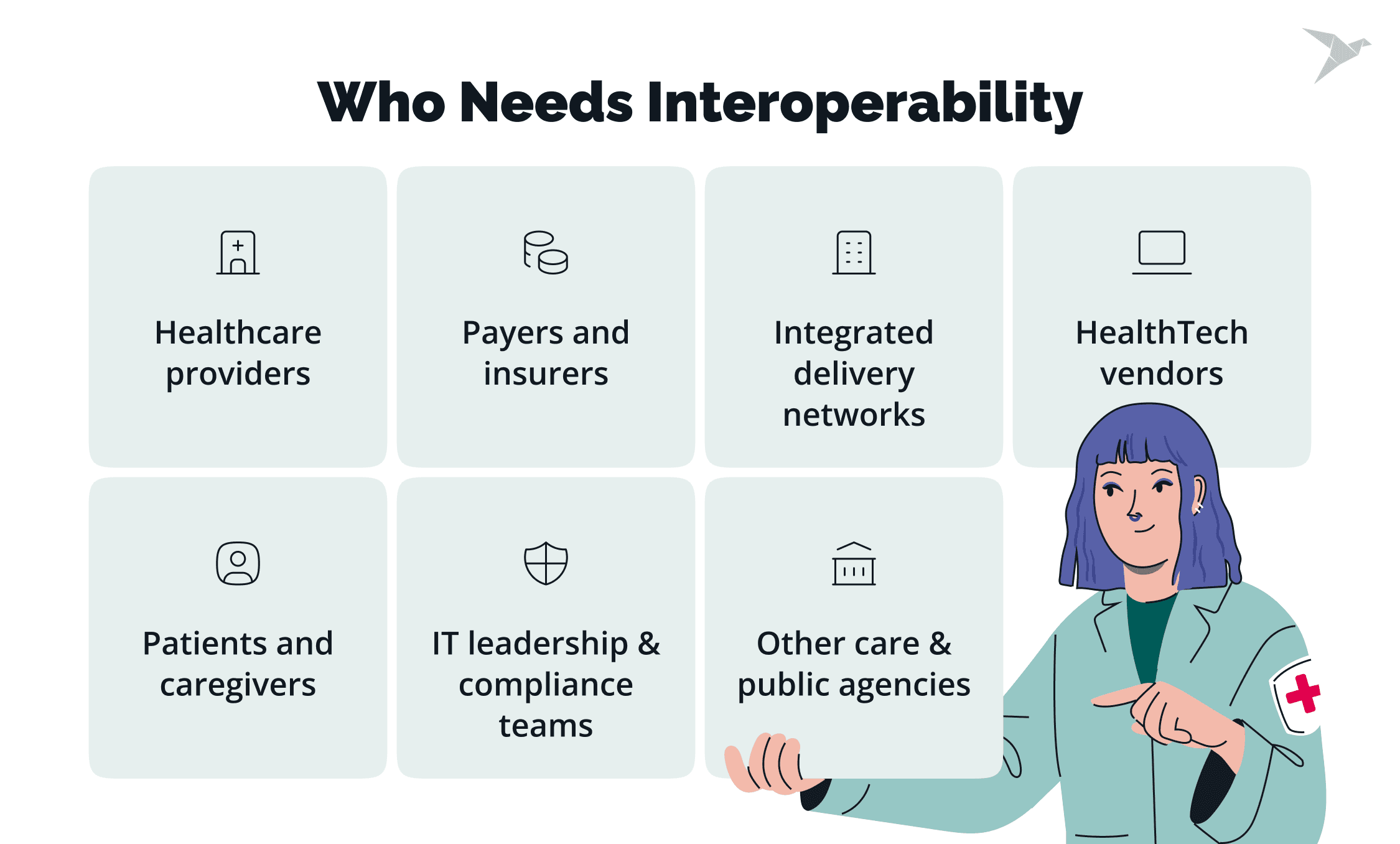
Interoperability is needed across the whole healthcare ecosystem, but the “why” changes by role: providers want safer care and less manual work, payers want automation and cost control, vendors want scalable integrations, IDNs want consistency across facilities, IT/compliance wants governed access, and patients want portable records they can trust.
💡 3 in 4 healthcare executives now rank data interoperability as a top or near-top priority for their organization, according to the Google Cloud and Fierce Healthcare industry survey.
Now let’s break it down in detail.
Healthcare providers
Providers need interoperability to keep care continuous and workable at the point of care, ensuring seamless access to a patient's medical history. That means external labs, imaging, meds, and history show up in the EHR in a usable way, so professionals aren’t re-entering data, repeating tests, or chasing information during referrals and transitions of care.
Interoperability reduces medical errors by providing accurate, up-to-date information and improves patient outcomes through better care coordination and informed decision-making. Without interoperability, health providers may have an incomplete understanding of an individual's or population's health needs, which leads to poorer outcomes and higher costs.
Payers and insurers
Payers need interoperability to reduce friction in claims, eligibility, and prior authorization, especially when decisions depend on structured clinical facts rather than attachments. Regulatory compliance, particularly for Medicaid services, is a key driver.
Federal requirements from CMS mandate that payers enable secure data exchange and support interoperability standards such as FHIR and APIs to facilitate the access and sharing of Medicaid-specific health data. Better data access also supports utilization management, population health, and faster detection of inconsistent or suspicious billing patterns.
HealthTech vendors
Vendors need interoperability to scale across customers without building custom interfaces for every EHR and partner. To achieve this, vendors must integrate with a wide range of information technology systems, including existing systems and disparate systems that often operate independently within healthcare organizations.
Strong interoperability shortens onboarding, lowers integration costs, and meets growing customer and regulatory expectations for standards-based access and auditability. However, many healthcare organizations face challenges due to outdated legacy IT systems that cannot easily integrate with newer solutions, which further complicates interoperability efforts.
Integrated delivery networks
IDNs need interoperability to operate as one system across multiple facilities and often multiple EHRs. To achieve this, IDNs must connect multiple systems and create interoperable systems that break down data silos, ensuring seamless data exchange and integration across electronic health records, imaging platforms, and other healthcare data management tools. It’s the backbone for cross-facility patient identity consistency, enterprise reporting, and value-based care workflows that depend on shared longitudinal data.
IT leadership and compliance teams
IT and compliance experts need interoperability that stays controlled: clear governance, least-privilege access, audit trails, and reliable integrations that don’t break quietly. Effective data management is essential for organizing, cleaning, and normalizing healthcare data, while regulatory compliance ensures that all data sharing and EHR systems meet privacy and security standards.
Foundational interoperability is the most basic level, which allows data to securely travel from one system to another and serves as a prerequisite for more advanced interoperability. Done right, it reduces operational risk instead of multiplying it.
Patients and caregivers
What makes healthcare interoperability important for patients and caregivers is that it enables their records to be accessible and portable. Timely and seamless portability of electronic health data ensures that information is exchanged efficiently and securely, enabling better access for both patients and caregivers. This leads to improved patient outcomes, as data flows more cleanly, patients repeat themselves less, decisions are made faster, and trust improves.
Next, let’s see what specific operational, clinical, and financial problems interoperability solves day to day.
HIPAA-compliant portal for secure medical data records and exchange

What Problems Does Interoperability Solve in Practice?
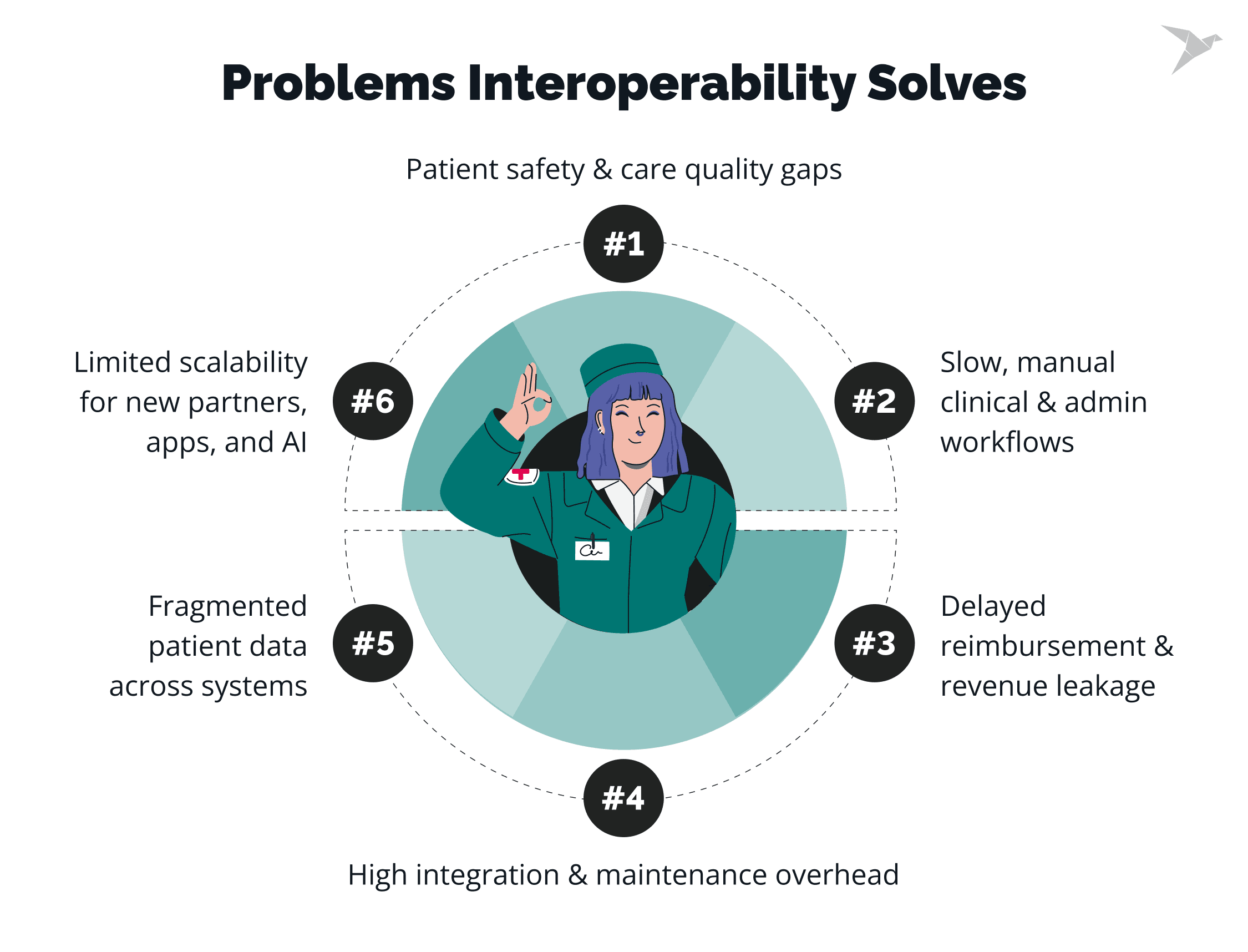
Interoperability solves a very practical problem: clinical, operational, and financial decisions depend on data that’s often split across systems, inconsistent, or late. When data can move reliably and land in a usable form, professionals waste less time, reduce risk, and avoid rebuilding integrations every time the organization changes. Now let’s look closer at the problems it addresses most often.
💡 The lack of true interoperability is costing the U.S. healthcare system around $30 billion per year in avoidable expenses, including redundant tests, manual rework, care delays, and errors that a seamless data flow could prevent.
Fragmented patient data across systems
Interoperability connects EHRs, labs, imaging, pharmacy, and external providers. Without it, clinicians lack context because data lives elsewhere, under a different identifier, or in an unusable format. The workaround is manual reconciliation: importing documents, copying values into notes, and rebuilding timelines. Strong interoperability brings data into the workflow consistently, so the chart reflects the patient, not system boundaries.
💡 Even when data is technically accessible, it often isn’t used effectively: 71% of hospitals said their clinicians had routine electronic access to outside patient's health records, yet only 42% reported that clinicians actually used that external data routinely in care, according to AHA.
Inefficient clinical and administrative workflows
Interoperability reduces repetitive work when systems can’t share reliable data. Demographics, insurance, orders, and summaries get re-entered because upstream data can't be trusted downstream. Clinical and billing workflows drift when documentation doesn't align with charge capture or payer needs, creating rework. Referrals, discharges, and care coordination also slow down when transfer is manual, untracked, or driven by calls and inbox follow-ups.
Patient safety and quality-of-care risks
Interoperability reduces safety gaps caused by missing or outdated information. Allergies, medications, recent results, and history often drop off when patients move across organizations or care settings. Inconsistent documentation adds risk when conditions are coded differently, or key context ends up in free text that downstream systems struggle to interpret. Delays matter as well. Late results, alerts, or discharge summaries force decisions without the full picture.
High integration and maintenance costs
Interoperability lowers the cost of brittle point-to-point interfaces. Custom integrations built per partner or workflow multiply quickly, each with its own mappings, edge cases, and failure modes. EHR upgrades and vendor changes then trigger regressions and incidents, pulling IT away from roadmap work. Standards-based contracts, reusable mappings, and centralized integration control reduce duplication and make change less expensive. A clean and secure data exchange schema also improves EHR ROI and data interoperability by reducing rework, denials, and integration overhead.
Delayed reimbursement and revenue leakage
Interoperability improves revenue cycle performance by moving consistent data from clinical systems into billing and payer workflows. Claims break when data is incomplete, inconsistent, or locked in unstructured formats, which leads to denials, resubmissions, and write-offs. Prior authorization and eligibility checks slow down when clinical evidence cannot be delivered quickly in a payer-ready format. Gaps between documentation and billing requirements also surface as missed charges, undercoding, and delayed submission.
Limited scalability and innovation
Improved interoperability supports growth and modernization. Adding a new partner, app, or care model becomes slow and risky when every connection requires custom work and tight coupling. Analytics, AI, and population health efforts stall when data can’t be normalized across sources or when provenance is unclear. Vendor lock-in grows as systems take on vendor-specific logic. Platform changes then require major rebuilds rather than controlled migrations.
Next, we’ll get specific about interoperability standards that matter in 2026.
Which Interoperability Standards Matter in 2026?
In 2026, interoperability relies on a small set of mature, widely adopted standards that are already proven in production. Organizations that want to understand how to achieve interoperability in the healthcare industry focus on standards with real ecosystem support, regulatory backing, and operational stability. Let’s look at the ones that actually matter.
HL7 v2
HL7 v2 remains the backbone of hospital and lab integrations. It’s still the most common way systems exchange admissions, discharges, transfers, orders, and results, especially inside hospitals and between hospitals and labs. HL7 v2 supports foundational interoperability as it enables basic data exchange between disparate health IT systems, and it also contributes to structural interoperability through standardized data formats that help organize and interpret information consistently.
Its strength is operational maturity: clinicians know how it behaves, vendors support it, and it runs reliably at scale. The limitation is flexibility. HL7 v2 messages vary widely by implementation, which makes reuse and standardization harder, especially when organizations try to modernize or extend beyond internal workflows.
HL7 FHIR
HL7 FHIR is the primary standard for modern healthcare APIs and application-level interoperability. It’s the foundation for patient access, data sharing with third parties, and many regulatory requirements tied to information access and non-blocking rules. FHIR’s strength comes from its resource-based model, REST APIs, and strong vendor adoption across major EHR platforms. In practice, FHIR is where most organizations start when they want to achieve interoperability in healthcare beyond traditional interfaces.
💡 The State of FHIR survey of health systems in 29 countries found that over 80% of them now have regulations requiring specific data exchange standards. In 65% of those cases, FHIR is explicitly mandated or recommended by the top health IT rules.
SMART on FHIR
SMART on FHIR defines how applications securely launch inside EHRs and access FHIR data with consistent authorization patterns. It’s the standard approach for embedding third-party apps into clinical workflows without custom security models for each integration. In 2026, many providers and vendors expect SMART support as a baseline requirement, especially for innovation ecosystems, clinical decision support, and patient-facing apps.
US Core and national FHIR profiles
FHIR, on its own, is flexible by design, which creates variability. National profiles like United States Core Data for Interoperability (USCDI) narrow that flexibility by defining which resources, fields, and terminologies must be supported for real-world interoperability. The USCDI establishes standardized health data classes and constituent data elements and ensures that healthcare systems can exchange information in a consistent and organized manner. These profiles are critical for regulatory alignment and consistent data exchange between organizations. Without them, two “FHIR-compatible” systems may still fail to interoperate in meaningful ways.
IHE profiles
IHE profiles focus on workflows rather than raw data models. They describe how standards like HL7, FHIR, and DICOM work together in real integration scenarios, such as imaging exchange, document sharing, and cross-enterprise care coordination. IHE remains common in environments where interoperability spans organizations, not just applications, and where predictable end-to-end behavior matters more than API design alone.
Terminology standards (SNOMED CT, LOINC, ICD)
Terminology standards are what make interoperability usable. SNOMED CT, LOINC, and ICD enable systems to agree on meaning, not just structure. They provide a shared vocabulary, facilitate semantic interoperability, and ensure that clinical and patient data are accurately represented and understood across different healthcare systems. In real implementations, terminology is often the hardest part: mapping legacy codes, handling local variations, and maintaining consistency over time. When organizations struggle with how to get interoperability in healthcare industry, terminology issues are often the root cause.
To address this gap, some organizations are also exploring language-first interoperability, an approach that focuses on aligning meaning and context before systems exchange data at scale.
Next, we’ll move from standards to structure and look at how to design an interoperability architecture that scales without locking you into fragile or vendor-specific solutions.
How Do You Design an Interoperability Architecture That Scales?
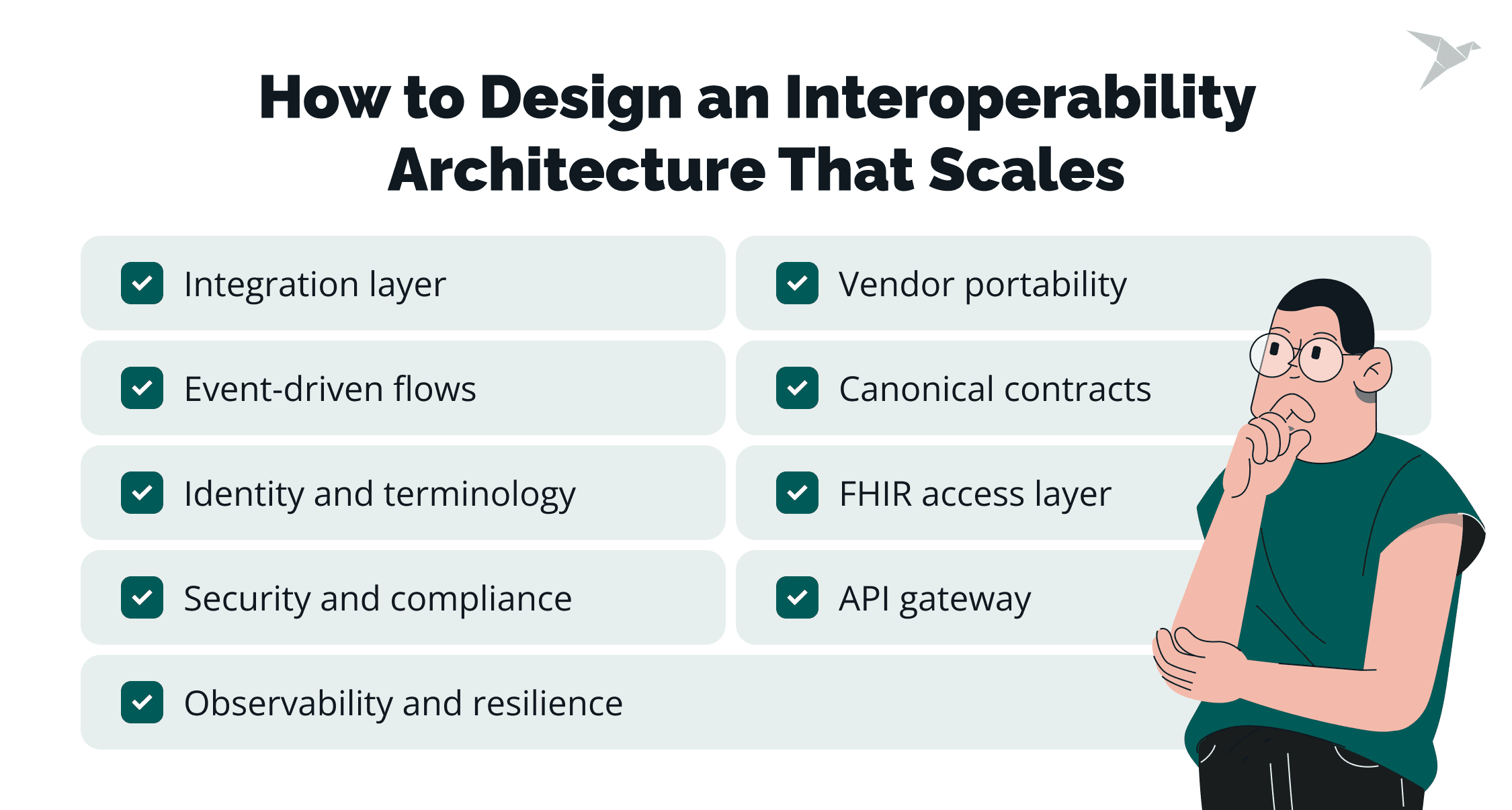
A scalable interoperability architecture separates concerns, standardizes access, and limits the blast radius of change. If you’re serious about how to achieve interoperability in healthcare industry, the goal is to build an architecture that survives new vendors, new regulations, and new care models without constant rework. Here’s what that looks like in practice.
Integration layer instead of point-to-point interfaces
A dedicated integration layer replaces fragile point-to-point connections with centralized routing, transformation, and policy enforcement. Instead of every system knowing how to talk to every other system, integrations flow through a controlled layer that handles mappings, validation, and rules consistently. This reduces duplication, lowers maintenance overhead, and keeps system changes from rippling unpredictably across the environment when one application evolves.
Strong healthcare integration practices reduce interface sprawl and make long-term interoperability easier to maintain.
API gateways and partner-facing API products
API gateways provide a consistent, governed entry point for external access. They handle authentication, throttling, versioning, and lifecycle management in one place, rather than scattering those concerns across services. Exposing partner-facing APIs as products, rather than one-off endpoints, creates predictable access patterns and shortens onboarding for apps, vendors, and affiliates, while keeping control firmly with the platform owner.
Event-driven integration for decoupling and real-time workflows
Event-driven patterns support real-time workflows without tight coupling between systems. Publishing events for admissions, results, notifications, or status changes allows consumers to react independently, rather than waiting on synchronous calls. This improves resilience during partial outages, smooths traffic spikes, and makes it easier to add new consumers without rewriting existing integrations.
Canonical model and contract-first design
A canonical data model creates stable internal contracts that are independent of vendor-specific formats. Contract-first design forces clarity around what data is exchanged and how it’s versioned before implementation begins. Reusable mappings across workflows reduce rework, and clear governance around breaking changes and backward compatibility prevents silent failures as systems evolve.
FHIR as an access and exchange layer
FHIR works best as a standardized access and exchange layer, not as a dumping ground for raw vendor data. A FHIR server or repository provides consistent APIs, while surrounding services handle validation, transformation, enrichment, and policy checks. Where appropriate, subscriptions and bulk data patterns support near–real-time updates and analytics use cases without overloading transactional systems.
Identity and terminology as foundational services
Identity and terminology can't be treated as afterthoughts. A clear patient identity strategy, often involving an MPI, keeps records aligned across systems, while consistent provider and facility identifiers support reliable attribution. Terminology normalization across LOINC, SNOMED CT, and ICD is what allows data to be compared, analyzed, and trusted across workflows and organizations.
Security and compliance architecture for interoperability
Security has to be embedded into the architecture, not layered on later. OAuth2, OIDC, and SMART patterns define consistent authorization, while consent management, auditing, and least-privilege access ensure compliance and traceability. Data segmentation and policy enforcement protect sensitive information without blocking legitimate access or slowing workflows.
Observability and operational resilience
Interoperability is operational infrastructure, so it needs observability. Observability helps break down data silos by providing visibility into how information flows between systems, which in turn improves operational efficiency and leads to better patient outcomes. Idempotency, retries, dead-letter queues, and replay mechanisms help integrations recover gracefully. Monitoring, tracing, and alerting across flows make failures visible early, and clear SLOs define what “working” actually means for critical data exchange paths.
Vendor-change resilience and portability patterns
Architectures that survive change isolate vendor-specific logic behind adapters and connectors. Automated regression and contract testing catch breaking changes early, before they reach production. Keeping core domain services free of vendor-specific assumptions preserves portability and reduces long-term lock-in.
Even with the right architecture in place, many organizations still struggle with execution time. Next, let’s look at the biggest interoperability implementation challenges and how to address them early.

What Are the Biggest Implementation Challenges?
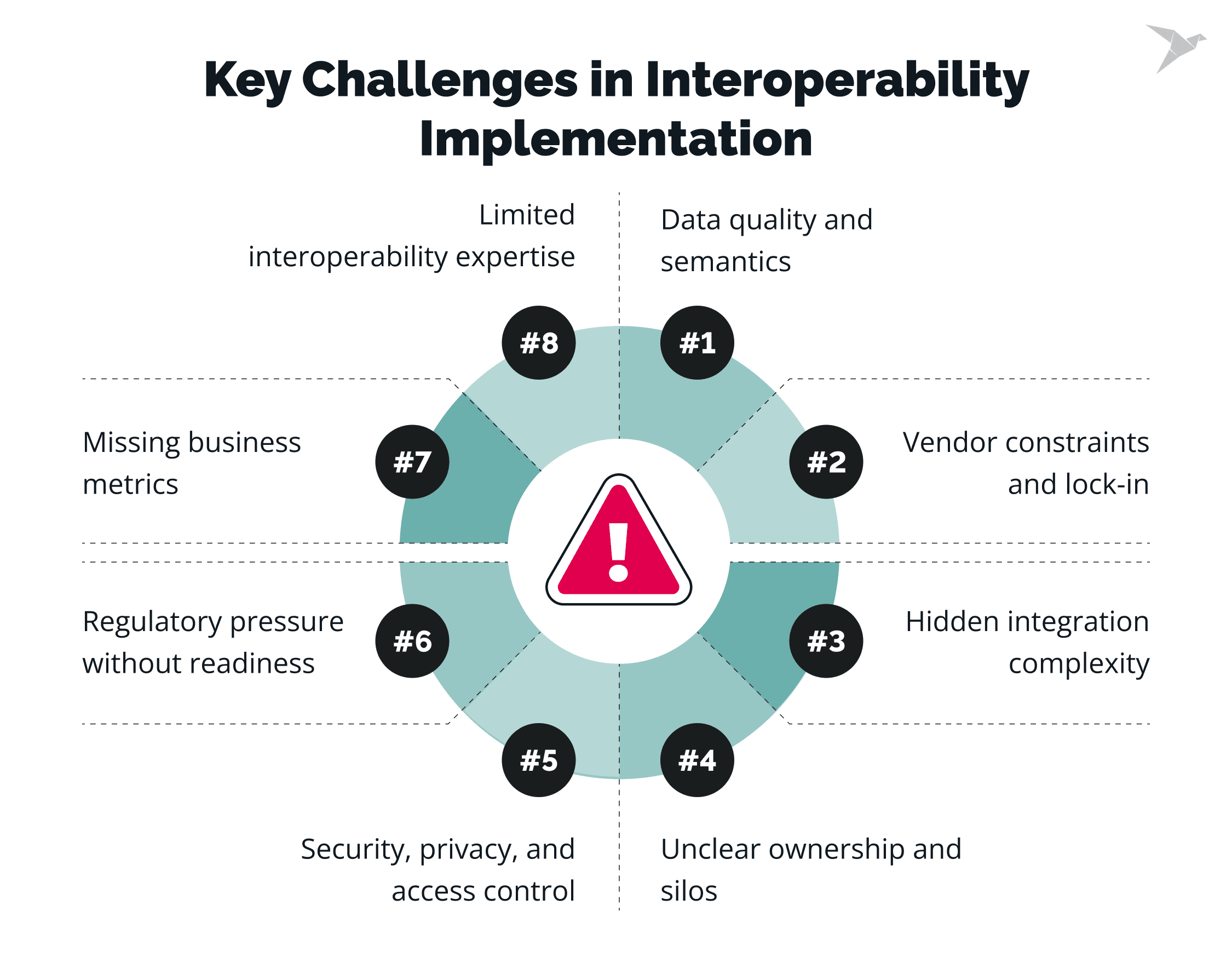
The biggest implementation challenges are data quality and semantics, vendor constraints, underestimated workflow complexity, unclear ownership, and security/compliance requirements. They usually surface after the pilot phase, when you scale. Organizations that plan for these early avoid rework, technical debt, and stalled rollouts. Now let’s look at each challenge and the most practical way to handle it.
Inconsistent data quality and semantics
Data quality issues slow interoperability more than any transport problem. Clinical documentation varies by system and by user, coding systems are applied inconsistently, and key fields are often missing or buried in free text. Normalization and validation then become ongoing, labor-intensive work instead of a one-time task. Organizations that succeed treat terminology mapping and data quality rules as shared services, with clear ownership, automated validation, and continuous monitoring rather than ad-hoc fixes.
💡 A 2024 HIMSS survey found only 53% of healthcare leaders were satisfied with their organization’s data quality management practices (the other 47% were unsatisfied).
Vendor-specific implementations and lock-in
Standards-based on paper doesn’t always mean standards-based in practice. Many EHRs and platforms implement FHIR or HL7 with vendor-specific constraints, optional fields, or undocumented behaviors. API limits, throttling rules, and upgrade cycles can quietly dictate what’s possible. The most resilient experts design against contracts, not vendors, isolating vendor logic behind adapters, testing against real behavior, and planning for breaking changes instead of reacting to them.
Underestimated integration complexity
Early pilots often look simple because they cover a narrow workflow with clean data. Complexity emerges later: edge cases across care settings, exceptions in clinical workflows, and dependencies between systems that weren’t obvious at the start. Scaling exposes performance limits and operational gaps. Organizations that anticipate this invest early in observability, error handling, and realistic test scenarios that mirror production.
Organizational silos and unclear ownership
Interoperability cuts across IT, clinical operations, compliance, security, and revenue cycle teams. When ownership is fragmented, decisions stall and priorities conflict. Projects drift because no one has authority to resolve trade-offs between speed, risk, and scope. Successful programs establish clear interoperability governance: defined decision rights, shared goals, and cross-functional accountability from the start.
Security, privacy, and access control constraints
Interoperability expands access, which raises legitimate security and privacy concerns. Consent rules vary by data type, jurisdiction, and use case, and access must stay aligned with least-privilege principles. Without clear patterns, organizations either over-restrict data or create risky exceptions. Strong implementations embed security into the architecture with consistent authorization models, auditable access, and tested incident response processes.
Regulatory pressure without technical readiness
Regulatory timelines often move faster than system readiness. Information blocking rules and patient access requirements push organizations to expose data quickly, sometimes before foundations are in place. Rushed implementations meet deadlines but accumulate technical debt that slows everything afterward. Companies that plan ahead separate compliance delivery from core architecture work, meeting requirements without compromising long-term stability.
Limited interoperability skills and experience
FHIR, HL7, healthcare security, and clinical workflows form a specialized skill set that’s still in short supply. Organizations often rely on generic integration tools or learn by trial and error, which stretches timelines and increases risk. Building internal expertise, supplementing with experienced partners, and documenting patterns early shortens the learning curve and improves consistency.
Lack of measurable business outcomes
Interoperability efforts often stall when they’re framed purely as technical projects. Without clear success metrics tied to clinical efficiency, reimbursement, risk reduction, or growth, it becomes hard to justify continued investment. Organizations that achieve consistent progress define outcomes early and track performance against them: reduced manual work, faster onboarding, fewer denials.
How Can TechMagic Help You Achieve Interoperability in Healthcare?
TechMagic helps you plan, build, and secure interoperability architecture. We combine healthcare software engineering with strong cybersecurity, so integrations don’t become your next risk area.
Here’s where we’re typically most useful:
- Interoperable, HIPAA-compliant solutions. We design and implement secure data exchange with the right access controls, audit trails, and monitoring from day one.
- Standards-based integrations. HL7 v2, where it still runs the hospital; FHIR and SMART on FHIR, where you need modern application programming interfaces and app ecosystems.
- Legacy modernization without a risky rebuild. We help you modernize old systems in steps so you can add interoperability layers, reduce interface sprawl, and keep operations stable.
- Architecture + delivery support. Interoperability strategy, reference architecture, hands-on implementation, testing, and stabilization when things get brittle.
If you want a clear plan for how to achieve interoperability in healthcare industry and an expert team that can build it securely, we’re ready to help!

Final Thoughts: What’s Next for Healthcare Interoperability
Healthcare interoperability in 2026 comes down to reliable, secure data that moves across systems and stays usable for care, operations, and compliance. Achieving true interoperability will transform healthcare by enabling seamless data exchange, which directly improves patient care through enhanced safety, reduced errors, and better health outcomes.
The path is consistent: use standards that work in production, build an architecture that scales past pilots, treat identity/terminology/security as foundations, and plan early for data quality, vendor constraints, governance, and measurable outcomes.
In the near future, patient access expectations and regulatory scrutiny will keep rising, pushing more API-first exchange and stronger auditability. AI will raise the bar too: cleaner data, clear provenance, consistent terminology, and predictable workflows. Interoperability will also shift toward product thinking: versioning, SLOs, monitoring, data integrity and security controls that survive vendor change.
Treat interoperability like long-term infrastructure, because it becomes exactly that once it’s live.
FAQ

Data exchange means systems can send and receive information. True interoperability means the receiving system can understand, trust, and use that data in workflows without manual cleanup. If clinicians still reconcile records by hand, you haven’t yet achieved interoperability in healthcare; you only move data. Interoperability in healthcare is often described in three levels: foundational interoperability (basic ability to send and receive data, such as emails or PDFs), structural interoperability (standardized data formats like FHIR and HL7 that ensure information is organized and consistent), and semantic interoperability (shared understanding of data so that information is meaningful and clinically accurate across different systems).
HL7 FHIR is not universally mandatory, but it is effectively required for patient access, third-party apps, and many regulatory use cases. Most organizations figuring out how to achieve interoperability in the healthcare industry rely on FHIR alongside existing standards like HL7 v2, not as a full replacement.
Initial interoperability use cases can take 3-6 months, while enterprise-scale programs often span 12-24 months, depending on data quality, vendor constraints, and governance. Organizations that treat it as long-term infrastructure move faster and avoid rework when they get interoperability in healthcare into production.

